|
|
|
|
|
|
|
|
|
|
|
|
|
RESEARCH IN PROGRESS
Torsional Ventricular Motion and What is the Clinical Significance? Frank A. Baciewicz Jr.,1 David G. Penney,2 William A. Marinelli,3 Ralph Marinelli4 James D. Stewart5 and Michael Duffy6
Cardiac and Thoracic Surgery, Wayne State University School of Medicine,1 Physicians observing heart motion on echocardiograms, during cardiac catheterization, or in the operating room, are impressed by the twisting or rotary motion of the left ventricle during systole. Conceptually, the heart has been treated as a pressure chamber. The rotary or torsional deformation has been poorly understood by basic scientists and has lacked clinical relevance. The extent of twisting, the regional variation in this phenomenon, and the relation to inotropic state, load conditions, heart rate, and disease state are just beginning to be understood. Recently, non-invasive imaging techniques have detected rotary blood flow in the ascending and descending aorta. Existence of this rotary blood flow and its possible relationship to ventricular torsional deformation is just starting to be explored. It has also been postulated that rotary blood flow is related to the geometry of the aorta and that die flow may be altered in certain disease states. This article reviews our current knowledge of ventricular twisting or torsional deformation and associated blood rotary motion. It attempts to answer the questions: (1) To what degree does ventricular twisting occur and where in the ventricle does it occur? (2) Is ventricular twisting related to ventricular fiber arrangement? (3) What is the functional and clinical significance of ventricular torsion? (4) Does rotary blood flow occur, and if so, when and where does it occur during the cardiac cycle? (5) Is rotary blood flow secondary to ventricular twist or forces within the blood vessels?
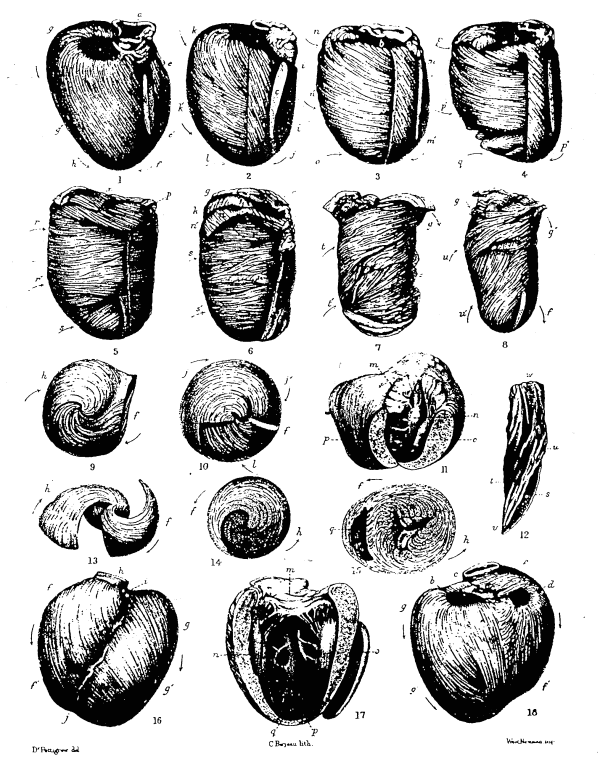
Ventricular Torsion Numerous techniques have been used to examine ventricular torsion. The early studies involved implanting radiopaque markers in the ventricular wall which could be imaged with cineradiography. More modern techniques, including echocardiography and magnetic resonance imaging, have allowed the ventricular wall to be marked non-invasively and its motion evaluated during the cardiac cycle. Cineradiography was used by Rushmer et al.1 who embedded short lengths of stainless steel wire in the heart wall of dogs and then studied the rotational motion. They noted rotation along the longitudinal axis of the heart not exceeding 10° McDonald2 used the same technique to measure rotational movement about the long axis, the most marked motion being at the beginning and end of systole. Prior to ejection, there was a slight counterclockwise rotation (looking from apex to base) of the epicardial surface which was accompanied by a small thrust of the apex toward the chest wall. During late systole, there was a slight clockwise rotation and retraction of the apex. Ingels et al3 implanted pure tantalum wire helices in the mid-wall of 24 patients during cardiac surgery and then used cineradiography to determine subsequent positions. He found that the equator of the left ventricle rotated minimally and the apical and basilar segments rotated in opposite directions. In the patients studied with biplane radiography, a wringing motion was observed during left ventricular contraction. The mean angle of twist was determined from the anterior and posterior wire helices marking the major transverse planes and the standard right anterior oblique projection plane. The angle was defined as positive if the anterior marker was higher than the corresponding posterior marker. The mean angle of twist at end diastole was -9.4° in the basal area and + 8.8° in the apical area. At end systole, the mean angles were -13.8° in die basilar area and +16.2° in the apical area, respectively. When computer analysis4 was added to the analysis of biplane cineradiography, it was noted that the base and apex twisted in opposite directions. The rotation was +13.2 ±4.0° at the apex, +3.4+1.0° at the equator and a -5.0 ± 13° at the base during systole. The mean twisting rates (relative to the base) at the apex were + 18°/sec during systole and -23°/sec during diastole. The directions and rates of torsional deformation were similar in these studies. In a study by Hansen et al5 ten heart transplant patients had tantalum markers implanted at the time of operation and were then studied with biplane cineradiography. Again, counterclockwise twisting around the left ventricular long axis was seen during systole. The torsional angles, relative to the base, were smaller in the anteroapical wall as compared to the inferior and lateral walls. Torsional angles at the mid-ventricular level were roughly half the angles exhibited at the apex. Torsional deformation of the anteroapical and inferior regions increased with tachycardia. The same investigators showed that dobutamine6 enhanced the torsional performance of the transplanted heart by 39% from 18.8 ± 8.2° to 26.1 ± 125°. Torsional deformation was insensitive to changes in end diastolic volume and only minimally sensitive to changes in end systolic pressure. This suggests that the torsional deformation of the left ventricle is a load-independent index of contractile state. More recent studies7 demonstrated a positive correlation between the grade of rejection and the degree of torsional deformation. The possibility of using the non-invasive parameter of torsional deformation to judge myocardial rejection is appealing. The use of echocardiography to assess heart torsion has the advantage that the myocardial-pericardial relationship is not disturbed. Miro et al8 utilized the papillary muscles as markers and displayed a minimal degree of counter-clockwise rotation ranging from 0-6° in 34 normal people. However, in patients with a secundum atrial septal defect, rotational deformation was exaggerated from 9-29° and surgical correction returned that value to the normal range. In the presence of valvular and ischemic disease, a decrease in left ventricular torsion was observed. Lorente et al9 using a combination of 2-dimensional echograms and cineangiography also reported average left ventricular apical rotation of 45° in 38 normal patients. Arts et al.10 studied left ventricular torsion in closed-chest dogs using echocardiography and. determined experimentally that the ventricular torsion was relatively constant over a wide range of preload, afterload, and contractility. Magnetic resonance imaging is another non-invasive method which can be used to assess myocardial motion. In fact, the precise motion of both endocardium and epicardium can be assessed using several tagging techniques. Zerhouni et al.11 showed increasing rotation of die heart from base to apex. Furthermore, he demonstrated a difference in the degree of rotation of die epicardial and endocardial sites suggesting individual contraction rates for the different muscle layers of the heart. Buchhalter12 and colleagues also used magnetic resonance imaging to show that the mean angle of torsion in the apical slice relative to the mean angle in the basilar slice in the endocardium was 19.1+2.0° counterclockwise when viewed from the apex. Epicardial torsion was 8.0 + 1.9° less than that in the endocardium. Torsion in the posteroseptal regions was less than the anteroseptal regions for both endocardium and epicardium, and the torsion angle increased with the distance from the base for both endocardium and epicardium. Clinical Correlation Sniderman et al13 noted an angular displacement of the ventricular apex of 5° toward the anterior wall in normal subjects. In those with right coronary artery lesions there was an apical displacement of 23° anterior or opposite to the ischemic zone. Six patients with coronary disease involving the left anterior descending coronary artery showed a similar abnormal pattern in the opposite direction. The changes in ventricular torsional deformation and corresponding changes toward normal after correction of secundum atrial septal defect have been noted previously. The possible implications for heart transplantation allograft rejection have been mentioned. Hansen7 has noted a change in the torsional deformation in the maximally deforming segment of 25% (from 21.1 ±15.2° to 16.0 ± 5.7°) during acute ejection as compared with the prerejection data. These episodes were confirmed by, endomyocardial biopsy. This change was associated with a significant decrease in peak systolic torsion rate, while the diastolic recoil rate was not changed. With successful treatment of me rejection episode, the torsional deformation returned to normal. Since the heart rate, mean arterial pressure, left ventricle end-diastolic pressure, stroke volume, and ejection traction were unchanged during these rejection episodes, the results of this study imply that ventricular torsional deformation may be a more sensitive, non-invasive indicator of left ventricular dysfunction and early rejection. Relationship to Cardiac Morphology The twisting motion of the heart is believed to be secondary to the arrangement of the muscle fibers. Pettigrew14 performed careful dissection of the heart of mammals and man, demonstrating 7 muscle layers. The three outer layers spiral with an increasing angle from the perpendicular, while the fourth layer is horizontal. The three inner layers spiral in the opposite direction, increasing toward the vertical. The layers are arranged in opposition so that 1 opposes 7, 2 opposes 6, and 3 opposes 5, with the fourth layer being a connecting layer. Pettigrew postulated that one triplet of muscles contracts during systole and the other stores energy that is utilized in diastole. In his view, the motion of the heart muscle is like that of a torsional pendulum. A reproduction of one of his anatomic dissections can be seen in Figure 1.
Myocardial fiber orientation was examined in the dog heart by Streeter et al15 He reported that there was a well-ordered distribution varying from 60° (from the circumferential axis with positive being toward the base) on the endocardium to approximately -60° on the epicardium of the heart. He found that this fiber angle increased in systole by approximately 7° near the base and 19° near the apex relative to their counterparts in diastole, suggesting a torsion during contraction of die left ventricle. More recently, Fernandez-Teran and Hurle16 confirmed that there are three muscle fiber layers in the heart wall based on orientation. They described superficial (subpicardial), middle and deep (subendocardial), muscle layers which are similar for both the left and right ventricle with the exception of the middle layer which is found only in the left ventricle. The opposing epicardial and endomyocardial muscle bundles might be important functionally. If potential energy is stored in these muscle fibers, the sudden release might promote filling during early diastole or the period of rapid ventricular filling. The proposed muscle bundles would also give a morphological correlate to the twisting or wringing motion of the left ventricle. Rotary Blood Flow Torsional motion of the left ventricle during systole and its recoil during diastole might impart .some rotational motion to the blood during contraction and ejection. In nature, fluids move in a spiral manner. This can be seen in whirlpools and when pouring water into a container. One postulate is that the structure of the cardiovascular system has developed to take full advantage of this natural propensity of fluids to spiral. A simple method to observe the tendency of fluids to spiral is to take a cone-shaped chamber and rotate it a few degrees in a fraction of a second. If a corked 6 1/2 oz. Perrier bottle (210 ml) containing 150 ml of water is given a snap of the wrist or an angular displacement of approximately 1° in 1 second, a vortex is produced. If a similar mechanism is working in the heart, that may be the cause of the rotary blood flow that has been detected in the aorta. Rotary Blood Flow in the Ventricle Rotation of the blood in the ventricle was detected by Doby and Lowman17 who used a radiopaque streamer technique. These studies demonstrated circular motion that persisted in the same direction throughout both systole and diastole. Irisawa et al18 injected 5% saline into the ventricle and observed incomplete mixing after one cardiac cycle in 92% of the trials. In 14%. mixing was incomplete even after four successive cardiac cycles. When the saline was injected into the left atrium, there still was incomplete mixing. Their work suggests streams of blood with different concentrations of saline swirling within the ventricle throughout systole and diastole. Experiments by Lynch and Bove19 using water-soluble radiopaque droplets and cineradiography observed currents in the canine heart with the predominant eddy involving the entire ventricular cavity and with movement toward the outflow tract. Major Arteries The studies by Lynch and Bove19 noted that radiopaque droplets cook a helical path in the aortic arch during systole. Studies by Segadal and Matre20 observed bi-directional flow in the ascending aorta from late systole to middle diastole, and blood appeared to rotate in a clockwise direction when observed from a left anterior position. Experimental studies21 with laminar flow of Newtonian fluids through curved pipes demonstrated vortex-like flow. When Yearwood and Chandran22 employed a human aortic arch model, they found that conventional laminar flow tended to become helical under pulsatile pressure and the influence of aortic curvature and tapering. This flow pattern was seen to originate in the ascending aorta. The helical flow was greatest near the inner wall and dissipated during diastole. They found the maximum rotary velocities to be 10-20% of the peak axial velocity. Talukder23 reported that coherent vortex structures in velocity waveforms occurred distal to mild constrictions (25-50% area reduction) of the dog aorta when examined with Doppler ultrasound and hot-film anemometry. In this situation rotary flow was associated with pulsatile flow through constrictions. Since the aortic valve is a constriction at the outflow tract of the left ventricle, it may be that this is a source of helical motion. Constrictions in the aorta may initially cause helical flow but with further progression of atherosclerotic disease in the major blood vessels, flow may become turbulent. The ability to diagnose helical blood flow may be a sensitive marker for atherosclerotic vascular disease. Farthing24 proposed that any vortex-like flow seen in the aortic arch is secondary to rotational blood flow emerging from the heart. He postulates this because vortex-like flow can only be created at a flow boundary and that such a boundary could not arise in the aorta. Based on his analysis, he believes that there must be rotating streams of blood within the ventricle. Bellhouse and Talbot25 have shown that vortices are generated in the aorta behind the aortic valve cusps when they are swept open in early systole. Given these data, Frazin's26 detection of rotational blood flow in the transverse aorta and proximal aorta with color-flow Doppler in 53 patients was exciting. Using a transesophageal color-flow Doppler, he demonstrated diastolic counterclockwise rotation and systolic clockwise helical flow in a high percentage of patients. This suggests that rotational flow begins in the aortic arch and is carried through the descending aorta where flow is asymmetric with systolic clockwise and diastolic counterclockwise elements. In a rebuttal editorial. Thomas27 suggested that the observed aortic clockwise and counterclockwise flow may be artifacts of the imaging technique. Magnetic resonance velocity mapping in the ascending and descending aorta of healthy patients has failed to demonstrate either rotary blood flow or turbulence.
Conclusion Studies to date indicate that the left ventricle undergoes a torsional deformation, twisting in a counterclockwise direction during systole and then returning in a clockwise direction during diastole. The degree of ventricular rotation appears to be altered in certain disease states such as secundum atrial septal defect, ischemic heart disease, and heart transplant rejection. It also appears that ventricular torsional deformation is sensitive to inotropic influences and heart rate, but is preload and afterload independent. The torsional. deformation is likely related to the myocardial anatomy as shown by Pettigrew. The opposing bands of muscle in the ventricular wall appear to be morphologically correlated with function. This review suggests that there is a rotational component in addition to the axial flow in the thoracic aorta and other large arteries. Whether this vortex-like flow is real is still subject to debate, but there are several mechanisms which could account for helical blood flow in the aorta. First, the torsional motion of the ventricle wall might cause the blood to vortex. Second, the structures projecting into the flowing blood stream at or above the aortic valve, and the curved form of the ascending, transverse and descending aorta may play a role. The presence and the clinical importance of rotary heart motion and blood flow still requires extensive investigation. The altered ventricular torsion in secundum atrial septal defect, ischemic heart disease, and heart transplant rejection offers an invitation into an area of heart motion which has not been explored. The pressure propulsion principle has been thought to be the basis for systolic ejection. If in fact rotary blood flow does exist in the ventricle and in the thoracic aorta. it could be postulated that the rotary flow assists ventricular ejection by means of momentum imparted from the vortex. The momentum transferring from this rotary blood motion could comprise a significant fraction of the total energy responsible for systolic ejection and blood flow through the aorta. The answer to this question and the relationship of torsional deformation of the ventricle to rotary blood flow in the arteries will be answered only by further experimental studies. References
|
|
Also by Ralph Marinelli:
The Heart is not a Pump: A
Refutation of the Pressure Propulsion Premise of Heart
Function,
Torsional Ventricular Motion and Rotary Blood Flow, What is the Clinical Significance? Galileo Versus Newton. |